
This post was co-authored by Wendy Wagner Robeson, Ed.D., Kimberly Lucas, Ph.D., and Kyle DeMeo Cook, Ph.D.
 As Massachusetts reels from losing millions of federal research dollars, it’s easy for us as research scientists to lose hope. It’s also easy to believe that with dwindling resources, we live in an even more dog-eat-dog world in which we must fight for the remaining grants and awards. But despite the challenges we are facing, we can choose to see this as a season of possibility—full of potential new ways to carry out our work that involve more collaboration, more partnership, and less competition.
As Massachusetts reels from losing millions of federal research dollars, it’s easy for us as research scientists to lose hope. It’s also easy to believe that with dwindling resources, we live in an even more dog-eat-dog world in which we must fight for the remaining grants and awards. But despite the challenges we are facing, we can choose to see this as a season of possibility—full of potential new ways to carry out our work that involve more collaboration, more partnership, and less competition.
Of course, researchers have long worked with colleagues and shared their findings with those in their field. But this particular moment—in which scientific research is under attack from the Trump administration—calls for much deeper collaboration: researchers must come together within, across, and even beyond our fields to determine what the real research questions are, identify whose skills are best suited to answer these questions, and design projects that produce data and information that our communities and policymakers can act upon.
We are ready to meet the moment: We are a group of early childhood policy researchers who are currently developing a statewide early childhood policy research collaborative in Massachusetts. We believe in a broad definition of “researcher”: included in our ranks are traditional academics; research scientists from think tanks; community-based measurement, evaluation, and learning professionals; government analysts; and participatory action practitioners from the field.
We recently held the first Massachusetts Early Childhood Policy Research Summit, at which we, alongside policymakers, advocates, funders, students, and practitioners, committed to working in coordination with each other. Together, we had over 100 participants and filled an entire day with discussion about the role of research, data, design, and collaboration in pushing our field forward. In her opening remarks, Rep. Alice Peisch noted her surprise at just how many researchers of all kinds want to work toward building a more collaborative network across the Commonwealth; those in the room agreed—we even surprised ourselves.
What does a research collaborative mean in practice? It means an annual summit and regular meetings of our leadership team, as well as several working groups focused on specific topics and methods of engaging the field. We decide as a group on our goals, mission, and values, taking into consideration the perspectives of researchers, practitioners, policymakers, and others across the field. We create a website and database of resources to keep our members connected. And, we think collectively about which projects to pursue, consider which of us is best positioned to pursue them, and strategize on how to get it all done and into the hands of those who can take action to support young children, families, and early educators across the Commonwealth of Massachusetts.
We are not the first to pursue this model. Similar early childhood policy research collaboratives exist in New York City, Chicago, New Hampshire and several other cities and states. In addition, the National Network of Education Research-Practice Partnerships (NNERPP) is a professional learning community that supports partnerships between researchers and education agencies in order to improve the relationships between research, policy, and practice. These partnerships are considered “a promising strategy for producing more relevant research, improving the use of research evidence in decision making, and engaging both researchers and practitioners to tackle problems of practice.” We agree that this is a promising strategy. It is far more effective for us to approach policymakers as a collaborative of more than 100 members than it is for us to approach them as individual researchers or even as individual institutions.
Does this kind of collaboration sound too good to be true? Certainly, there are challenges to working collaboratively in this way, especially when you’re forming partnerships across research institutions. People have to be willing to move out of their silos and out of the mindset of competition, which most of us have been in our entire careers as we competed against each other for grants, projects, and awards. Another challenge is simply finding the time to collaborate—to meet with each other, to build trusting relationships, and to work through difficult conversations.
But despite these challenges, we all understand that when funding opportunities are limited—and when the problems we aim to address persist—we can’t waste time and money unnecessarily replicating each other’s work or competing for the benefit of our individual institutions. This summer, we expanded our leadership team and supported a working group to keep up the momentum and ensure that collaboration is built into the design of our work together; we were 25 individuals representing 19 colleges and universities, research firms, government agencies, and direct service organizations. We’re excited to continue our work into next year—and to welcome many more researchers, data analysts, and designers of all walks to our 2026 summit.
In order to continue work that can positively impact children, families, and communities in Massachusetts, we must work together. We are ready.
Wendy Wagner Robeson, Ed.D., is a Senior Research Scientist at the Wellesley Centers for Women. Kimberly Lucas, Ph.D., is Professor of the Practice in Public Policy and Economic Justice in the School of Public Policy and Urban Affairs at Northeastern University. And Kyle DeMeo Cook, Ph.D., is Clinical Assistant Professor at Wheelock College of Education and Human Development at Boston University.
As Massachusetts reels from losing millions of federal research dollars, it’s easy for us as research scientists to lose hope. It’s also easy to believe that with dwindling resources, we live in an even more dog-eat-dog world in which we must fight for the remaining grants and awards. But despite the challenges we are facing, we can choose to see this as a season of possibility—full of potential new ways to carry out our work that involve more collaboration, more partnership, and less competition.Of course, researchers have long worked with colleagues and shared their findings with those in their field. But this particular moment—in which scientific research is under attack from the Trump administration—calls for much deeper collaboration: researchers must come together within, across, and even beyond our fields to determine what the real research questions are, identify whose skills are best suited to answer these questions, and design projects that produce data and information that our communities and policymakers can act upon.
We are ready to meet the moment: We are a group of early childhood policy researchers who are currently developing a statewide early childhood policy research collaborative in Massachusetts. We believe in a broad definition of “researcher”: included in our ranks are traditional academics; research scientists from think tanks; community-based measurement, evaluation, and learning professionals; government analysts; and participatory action practitioners from the field.
We recently held the first Massachusetts Early Childhood Policy Research Summit, at which we, alongside policymakers, advocates, funders, students, and practitioners, committed to working in coordination with each other. Together, we had over 100 participants and filled an entire day with discussion about the role of research, data, design, and collaboration in pushing our field forward. In her opening remarks, Rep. Alice Peisch noted her surprise at just how many researchers of all kinds want to work toward building a more collaborative network across the Commonwealth; those in the room agreed—we even surprised ourselves.
What does a research collaborative mean in practice? It means an annual summit and regular meetings of our leadership team, as well as several working groups focused on specific topics and methods of engaging the field. We decide as a group on our goals, mission, and values, taking into consideration the perspectives of researchers, practitioners, policymakers, and others across the field. We create a website and database of resources to keep our members connected. And, we think collectively about which projects to pursue, consider which of us is best positioned to pursue them, and strategize on how to get it all done and into the hands of those who can take action to support young children, families, and early educators across the Commonwealth of Massachusetts.
We are not the first to pursue this model. Similar early childhood policy research collaboratives exist in New York City, Chicago, New Hampshire and several other cities and states. In addition, the National Network of Education Research-Practice Partnerships (NNERPP) is a professional learning community that supports partnerships between researchers and education agencies in order to improve the relationships between research, policy, and practice. These partnerships are considered “a promising strategy for producing more relevant research, improving the use of research evidence in decision making, and engaging both researchers and practitioners to tackle problems of practice.” We agree that this is a promising strategy. It is far more effective for us to approach policymakers as a collaborative of more than 100 members than it is for us to approach them as individual researchers or even as individual institutions.
Does this kind of collaboration sound too good to be true? Certainly, there are challenges to working collaboratively in this way, especially when you’re forming partnerships across research institutions. People have to be willing to move out of their silos and out of the mindset of competition, which most of us have been in our entire careers as we competed against each other for grants, projects, and awards. Another challenge is simply finding the time to collaborate—to meet with each other, to build trusting relationships, and to work through difficult conversations.
But despite these challenges, we all understand that when funding opportunities are limited—and when the problems we aim to address persist—we can’t waste time and money unnecessarily replicating each other’s work or competing for the benefit of our individual institutions. This summer, we expanded our leadership team and supported a working group to keep up the momentum and ensure that collaboration is built into the design of our work together; we were 25 individuals representing 19 colleges and universities, research firms, government agencies, and direct service organizations. We’re excited to continue our work into next year—and to welcome many more researchers, data analysts, and designers of all walks to our 2026 summit.
In order to continue work that can positively impact children, families, and communities in Massachusetts, we must work together. We are ready.
Wendy Wagner Robeson, Ed.D., is a Senior Research Scientist at the Wellesley Centers for Women. Kimberly Lucas, Ph.D., is Professor of the Practice in Public Policy and Economic Justice in the School of Public Policy and Urban Affairs at Northeastern University. And Kyle DeMeo Cook, Ph.D., is Clinical Assistant Professor at Wheelock College of Education and Human Development at Boston University.



 Sex education in the American public school system varies from state to state and from school district to school district. The lack of standardized sex education makes family education and conversations about sex and relationships all the more important for teenagers and their development. It is often assumed that parents are the default—that they are the only family members responsible for initiating these conversations. In my research conducted with WCW Senior Research Scientist
Sex education in the American public school system varies from state to state and from school district to school district. The lack of standardized sex education makes family education and conversations about sex and relationships all the more important for teenagers and their development. It is often assumed that parents are the default—that they are the only family members responsible for initiating these conversations. In my research conducted with WCW Senior Research Scientist  The pandemic has altered family life in unexpected ways.
The pandemic has altered family life in unexpected ways. 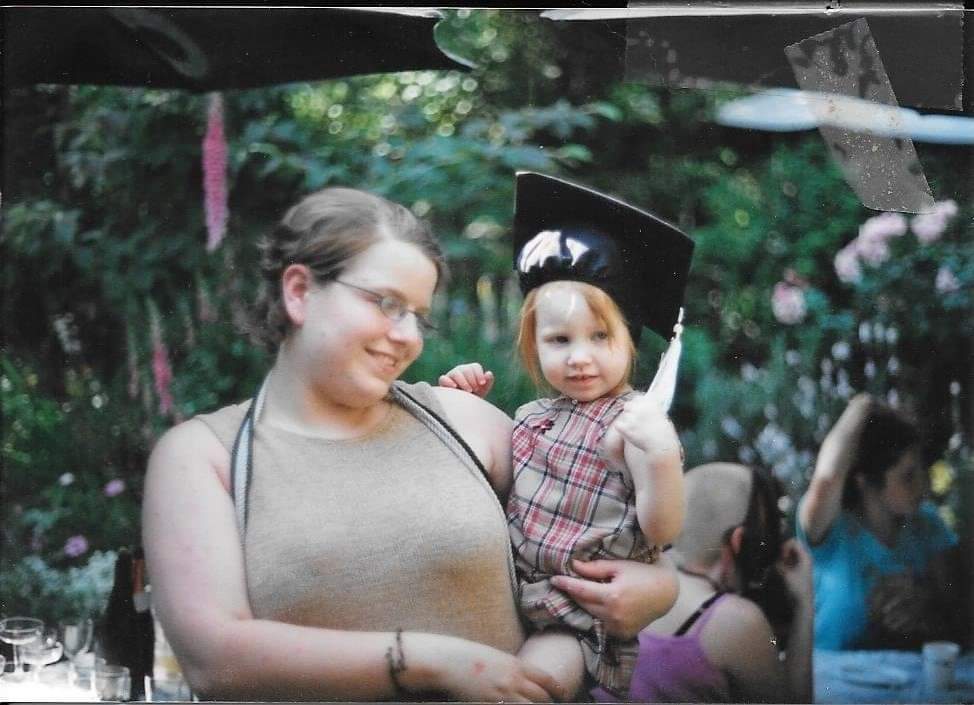 Last year on Mother's Day, I was driving through the Rocky Mountains, on my way from Oregon to Maine where my life was about to change forever. It was the first Mother's Day I had spent without my kids since they were born, and the first Mother's Day since my own mother had passed away. I yearned to call her to share the news of my latest adventure, as I always had during our frequent long-distance phone chats, but I knew I couldn’t. The following week, my daughter would bring my granddaughter into the world on the southern coast of Maine. The transcontinental journey I was on would end with the newest love of my life joining our family.
Last year on Mother's Day, I was driving through the Rocky Mountains, on my way from Oregon to Maine where my life was about to change forever. It was the first Mother's Day I had spent without my kids since they were born, and the first Mother's Day since my own mother had passed away. I yearned to call her to share the news of my latest adventure, as I always had during our frequent long-distance phone chats, but I knew I couldn’t. The following week, my daughter would bring my granddaughter into the world on the southern coast of Maine. The transcontinental journey I was on would end with the newest love of my life joining our family.
 Although these are all big questions, I have at least learned a few things over the years through my
Although these are all big questions, I have at least learned a few things over the years through my  Lisa Fortuna
Lisa Fortuna

 In the last couple of years, more research has surfaced regarding LGBTQ elderly people, which provides a sobering look at their attitudes and thoughts about aging. The first and obvious concern is aging in a society and community that places a high value on youth, leaving the elderly feeling useless and insignificant (Fox, 2007). This is both within the LGBTQ communities and in the general population. Ageism is pervasive in the U.S.
In the last couple of years, more research has surfaced regarding LGBTQ elderly people, which provides a sobering look at their attitudes and thoughts about aging. The first and obvious concern is aging in a society and community that places a high value on youth, leaving the elderly feeling useless and insignificant (Fox, 2007). This is both within the LGBTQ communities and in the general population. Ageism is pervasive in the U.S.
 Vita Sackville-West
Vita Sackville-West
 It’s important to talk with teens before they have sex. Research tells us that it is critical for teens to learn about sexual issues from a trusted adult before they have sex.
It’s important to talk with teens before they have sex. Research tells us that it is critical for teens to learn about sexual issues from a trusted adult before they have sex.
 human nervous system is literally wired to function best when in
human nervous system is literally wired to function best when in 
 wear away at our health and wellbeing. The NPR poll found that individuals with a chronic illness were more likely to report high stress in the previous month (36% compared to 26% overall), as were individuals living in poverty (36%) and single parents (35%). These chronic stressors tax our abilities to cope with stress. For those individuals with high levels of stress, problems with finances was one of the main sources of stress, and this was especially true for those
wear away at our health and wellbeing. The NPR poll found that individuals with a chronic illness were more likely to report high stress in the previous month (36% compared to 26% overall), as were individuals living in poverty (36%) and single parents (35%). These chronic stressors tax our abilities to cope with stress. For those individuals with high levels of stress, problems with finances was one of the main sources of stress, and this was especially true for those 
 Media coverage about social media has not been kind—often linking its use with cyberbullying, sexual predators, and depression or loneliness. But recent scholarship on new media demonstrates that interpersonal communication, online and offline, plays a vital role in integrating people into their communities by helping them build support, maintain ties, and promote trust. Social media is often used to escape from the pressures of life and alter moods, to secure an audience for self-disclosures, and to widen social networks and increase social capital. The
Media coverage about social media has not been kind—often linking its use with cyberbullying, sexual predators, and depression or loneliness. But recent scholarship on new media demonstrates that interpersonal communication, online and offline, plays a vital role in integrating people into their communities by helping them build support, maintain ties, and promote trust. Social media is often used to escape from the pressures of life and alter moods, to secure an audience for self-disclosures, and to widen social networks and increase social capital. The 
 In Mississippi, advocacy for low-income women and children tends to occur only in the non-profit and non-governmental sectors, which are both relatively under-resourced in comparison with other states. No adequately powerful counter-voice exists to offset the public tone of hostility toward low-income women. Further, conscious and sub-conscious racism is so entrenched in Mississippi that even policies that would appear to address racial discrimination turn out to have no impact. Mississippi could be said to be “Ground Zero” for structural racism. So intractable is this form of racism at all class levels that the elimination of
In Mississippi, advocacy for low-income women and children tends to occur only in the non-profit and non-governmental sectors, which are both relatively under-resourced in comparison with other states. No adequately powerful counter-voice exists to offset the public tone of hostility toward low-income women. Further, conscious and sub-conscious racism is so entrenched in Mississippi that even policies that would appear to address racial discrimination turn out to have no impact. Mississippi could be said to be “Ground Zero” for structural racism. So intractable is this form of racism at all class levels that the elimination of 
 Utilizing such “rape myths” like the need for well-lit streets and women’s ability to walk safely perfectly illustrates Haugen’s limited understanding of sexual violence:
Utilizing such “rape myths” like the need for well-lit streets and women’s ability to walk safely perfectly illustrates Haugen’s limited understanding of sexual violence: 
 But for a single mother, even this culturally permissible deviance is insufficient. My life with Amy is different from the lives of most of my colleagues and friends. I could not provide emotional, physical and financial support for Amy without re-envisioning motherhood. Amy and I have lived with a shifting assortment of male and female students, single women as well as married women with children. Work for me is not possible without round the clock care for Amy. This is true for all mothers and children, but it is a need that is normally outgrown. Not so in our case. Amy fuels my passion for feminist solutions; not simply for childcare, but for policy issues across the board. I know first hand too many of the dilemmas confronting women, from the mostly invisible, predominately female workers who care for others in exchange for poverty level wages to successful business women struggling to be perfect mothers, perfect wives and powerfully perfect CEOs.
But for a single mother, even this culturally permissible deviance is insufficient. My life with Amy is different from the lives of most of my colleagues and friends. I could not provide emotional, physical and financial support for Amy without re-envisioning motherhood. Amy and I have lived with a shifting assortment of male and female students, single women as well as married women with children. Work for me is not possible without round the clock care for Amy. This is true for all mothers and children, but it is a need that is normally outgrown. Not so in our case. Amy fuels my passion for feminist solutions; not simply for childcare, but for policy issues across the board. I know first hand too many of the dilemmas confronting women, from the mostly invisible, predominately female workers who care for others in exchange for poverty level wages to successful business women struggling to be perfect mothers, perfect wives and powerfully perfect CEOs.
 Treating youth depression once it emerges may be much more distressing, and much less effective, than identifying early symptoms of illness and treating them before they develop into a full-blown disorder. Prevention approaches have the potential to reach a large number of adolescents, and may be more acceptable than treatment because services can be rendered in non-clinical settings (e.g., schools, primary care settings), and do not require adolescents to identify themselves as ill.
Treating youth depression once it emerges may be much more distressing, and much less effective, than identifying early symptoms of illness and treating them before they develop into a full-blown disorder. Prevention approaches have the potential to reach a large number of adolescents, and may be more acceptable than treatment because services can be rendered in non-clinical settings (e.g., schools, primary care settings), and do not require adolescents to identify themselves as ill.
 When I was 39, I gave birth to my daughter. I took a few months off with her, using up most of my sick leave, because this was pre-Family Medical Leave Act, and Wellesley College did not yet have paid parental leave. While at home, I discovered that parenthood was hard work, work that required a different rhythm than my paid work.
When I was 39, I gave birth to my daughter. I took a few months off with her, using up most of my sick leave, because this was pre-Family Medical Leave Act, and Wellesley College did not yet have paid parental leave. While at home, I discovered that parenthood was hard work, work that required a different rhythm than my paid work.
 While
While 
 So, where are all the people with mental illness? From what I hear in my office, many are hiding and suffering in silence for fear of being stigmatized, pitied, or seen as weak. American, Westernized culture plays a large role in this fear. The pervasive image of an American is a person who is strong, independent, and can
So, where are all the people with mental illness? From what I hear in my office, many are hiding and suffering in silence for fear of being stigmatized, pitied, or seen as weak. American, Westernized culture plays a large role in this fear. The pervasive image of an American is a person who is strong, independent, and can 
 What are some cheap nutritious foods? In no particular order, the Biro family’s diet last week consisted of rice, beans, potatoes, inexpensive meat (specifically split chicken breasts on sale, and stew meat on sale), bananas, eggs, carrots (but you have to peel them yourself--having the factory do the work for you and turn them into baby carrots costs too much), pasta, homemade pancakes, nuts, oatmeal and super cheap granola bars we bought in bulk (more on this later). We bought a small crate of “Clementine” oranges on sale for $6, or $0.20 apiece. We made homemade pizza one night, with dough from scratch costing roughly $0.40, the sauce about $1 and mozzarella at $3, totaling not quite $5 for 2 pizzas, with leftovers for lunch. We did buy fresh broccoli, which is expensive at $0.30 per serving, so we didn’t have much. Frozen vegetables are usually cheaper, but not always. Lentils are cheap and high-quality calories but we didn’t get those in.
What are some cheap nutritious foods? In no particular order, the Biro family’s diet last week consisted of rice, beans, potatoes, inexpensive meat (specifically split chicken breasts on sale, and stew meat on sale), bananas, eggs, carrots (but you have to peel them yourself--having the factory do the work for you and turn them into baby carrots costs too much), pasta, homemade pancakes, nuts, oatmeal and super cheap granola bars we bought in bulk (more on this later). We bought a small crate of “Clementine” oranges on sale for $6, or $0.20 apiece. We made homemade pizza one night, with dough from scratch costing roughly $0.40, the sauce about $1 and mozzarella at $3, totaling not quite $5 for 2 pizzas, with leftovers for lunch. We did buy fresh broccoli, which is expensive at $0.30 per serving, so we didn’t have much. Frozen vegetables are usually cheaper, but not always. Lentils are cheap and high-quality calories but we didn’t get those in. 